
Colon Disease Diseases & Treatment Options
Diseases of the colon
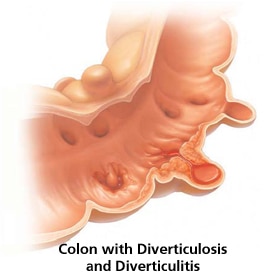
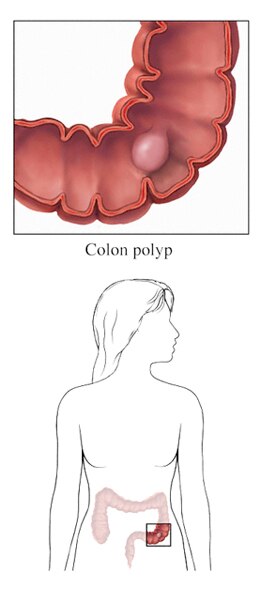
Several diseases can interfere with the normal functioning of the colon. These diseases can have various effects and are traditionally classified as benign (non-cancerous) or malignant (cancerous) and can cause various symptoms including bleeding, infection, and perforation.
In some cases, doctors treat the disease by removing a segment of the colon. Given that the average human has 8-10 feet of small bowel and 3-5 feet of colon, removal of a segment will generally not effect normal functioning of the colon.
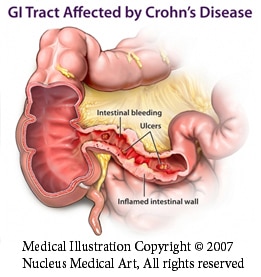
Crohn’s Disease and Ulcerative Colitis
Background: Inflammatory Bowel Disease (IBD) includes Crohn’s Disease and Ulcerative Colitis
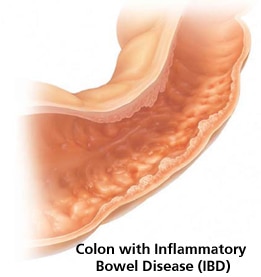
- Inflammatory bowel disease (IBD) is caused by chronic inflammation of the intestinal tract. There are two forms of inflammatory bowel disease: Crohn’s disease and ulcerative colitis (UC).
- Crohn's disease and ulcerative colitis are similar — so similar that they're often mistaken for one another. Both disease cause inflammation of the lining of your digestive tract, and both may result in severe bouts of diarrhea and abdominal pain.
- Crohn's disease can occur anywhere in your digestive tract, often spreading deep into the layers of affected tissues. Ulcerative colitis, on the other hand, usually affects only the innermost lining of your large intestine (colon) and rectum.
Clinical Presentation: What are the common signs and symptoms of inflammatory bowel disease?
Patients with inflammatory bowel disease could present with any of the following:
- abdominal pain
- nausea, vomiting
- diarrhea, bloody stools
- weight loss or weight gain
- various associated complaints or diseases, often autoimmune disorders (arthritis, skin lesions, and liver and bile duct disorders).
In Crohn’s disease, inflammation causes cells in the affected areas of your intestine to secrete large amounts of water and salt. Because the colon can't absorb this excess fluid, you develop diarrhea. Altered intestinal contractions also can contribute to loose stools. Diarrhea can range from mild to severe.
Diarrhea can also be a symptom of ulcerative colitis. However, patients with ulcerative colitis tend to experience bloody diarrhea and also something called tenesmus. Tenesmus is the sensation of having to move ones’ bowels.
Food moving through your digestive tract can cause inflamed tissue to bleed, and your bowel may also bleed on its own. You might notice bright red blood in the toilet bowl or darker blood mixed with your stool. Should this occur, you must notify your physician.
Treatment: What needs to be done if I have inflammatory bowel disease?
Medical Therapy:
- Usually, treatment of inflammatory bowel disease begins with medical therapy. Most commonly, treatment of inflammatory bowel disease requires mesalamine or Asacol® (mesalazine), which in part also acts as an anti-inflammatory agent.
- Depending on the level of severity, inflammatory bowel disease may require immunosuppression to control the symptoms. Immunosupression refers to using medications to depress the body’s ability to generate an inflammatory response. Such medications often used include azathioprine, methotrexate, or 6-mercaptopurine. If initial treatment is unsuccessful, a combination of the aforementioned immunosupression drugs may or may not be administered, depending on the patient.
- During times of acute exacerbation of inflammatory bowel disease, steroids are often used to control disease flares. Remicade® (infliximab), another type of anti-inflammatory, has been used for many years in Crohn’s disease and more recently also in patients with ulcerative colitis.
- Severe cases may require surgery, such as bowel resection of the diseased portion of intestines, and/or temporary or permanent colostomy or ileostomy.
Surgical Therapy: Crohn’s Disease
- Surgery for Crohn’s disease is recommended in carefully selected cases because the disease can recur in any remaining portion of the gastrointestinal tract.
- Surgery is recommended when Crohn’s related complications occur. This includes infection (abscess), perforation, blockage or obstruction and possible fistula (connection between bowel and other structures).
Surgical Therapy: Ulcerative Colitis

- Of the two conditions, patients with ulcerative colitis are more likely to undergo surgery because removal of the colon and rectum will cure the disease.
- Surgery for ulcerative colitis usually entails removing the entire colon. There are different ways to remove the colon as well as different ways to put the colon back together.
- The surgery that was traditionally performed for ulcerative colitis was a proctocolectomy which removed the entire colon, rectum and anus. However, this operation required the creation of an ileostomy. This is an opening in the small intestine that is brought up to the skin where waste is expelled. This opening requires a bag to be worn over the opening in the skin to collect waste.
- Another surgical option would be to create an ileostomy with an internal pouch that acts as a collecting system. This eliminates the need for a bag; however, the opening in the skin still exists. Defecation is maintained by the patient on a schedule.
- A different surgical approach would be to only remove the large intestine (colon) leaving the rectum and anus. The small intestine (ileum) would then be connected to the rectum. This relieves the patient of having to live with a colostomy but leaves large intestine behind that may be susceptible to recurrent ulcerative colitis. Thus, frequent surveillance colonoscopy is required.
- A newer and more appealing surgical procedure is called an Ileo-anal J pouch. This operation removes the large intestine and rectum but leaves the anus. The small intestine is then connected to the anus and fashioned into a pouch capable of storing feces.
- Most of these operations can be done either open or laparoscopically. Laparoscopic surgery for ulcerative colitis has shown similar long term outcomes when compared to open surgery. As with other types of minimally invasive surgery, laparoscopic surgery usually results in shorter hospital stays and shorter recoveries.
- It is important to note that not all procedures can be done laparoscopically and the decision should always be discussed between patient and surgeon.
Risks of surgery for ulcerative colitis:
The risks of any surgery must be weighed against the risks associated with disease state requiring the intervention.
In the case of ulcerative colitis, the risks of ongoing inflammation, infection and subsequent colon cancer are sometimes greater than the risks described below and surgery is thus indicated.
Major risks of laparoscopic proctocolectomy with ileoanal J pouch for ulcerative colitis can include but are not limited to:
- Wound infection (1-3%) possibly requiring opening of wound, drainage, antibiotics and prolonged wound care.
- Abdominal cavity infection (1-3%) possibly requiring antibiotics, drainage of the infection via a catheter or re-operation to drain the infection.
- Leakage from the re-connection points (anastomotic leak) (5-10%) resulting in infection and possibly drainage of the infection via a catheter or re-operation to drain the infection. Re-operation may also require creation of a temporary colostomy to allow the body time to heal the infection. This can typically be reversed 4-6 months later.
- Bleeding from surgical sites (1-3%) requiring observation, blood transfusion or re-operation.
- Pouchitis or inflammation of the J pouch (25%) with subsequent diarrhea and possible leakage of mucous and stool from the anus.
Information on this site should not be used as a substitute for talking with your doctor. Always talk with your doctor about diagnosis and treatment information.